Mutation/technique illustrated:
Point mutation generating loss of restriction site detected by Southern blot and RFLP; mutated fragment is larger.
The DNA sequence files are the human beta globin gene, on chromosome 11, locus HUMHBB from GenBank, 73,308 bp. To create the sickle cell mutation, nucleotide 62206 was changed from A to T. The probe corresponds to nucleotides 61023 to 61210 and hybridizes to the fragment which will be larger if the MstII site is eliminated by the mutation at position 62206. The enzyme MstII recognizes the site CATNAGG, where N can be either A, C, T, or G. The Case It! program searches sequentially for each of these 4 forms of the restriction enzyme, and cuts the sequences accordingly.
Based on Fig. 27-9 in Watson et al., Recombinant DNA, 2nd ed., Scientific American Books, 1992.
Case A:
Steve and Martha are expecting their second child. They know that sickle cell disease runs in both of their families. They want to know whether this child could be affected. Neither they nor their 10-year-old daughter, Sarah, have shown any symptoms of the disease. They decide to have DNA tests to determine the status of the fetus, as well as to find out whether they in fact are carriers of the disease gene.
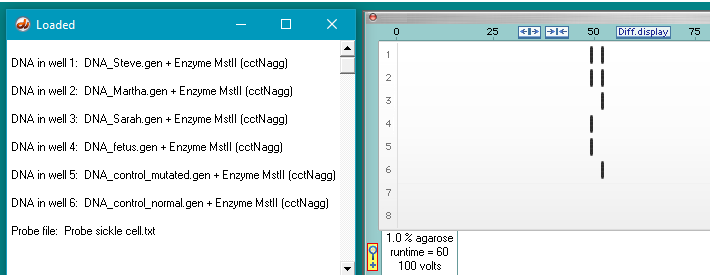
- Steve (father) – heterozygous (carrier)
- Martha (mother) – heterozygous (carrier)
- Sarah (daughter) – homozygous normal
- Fetus – homozygous sickle (affected)
- Control DNA, homozygous for sickle cell mutation
- Control DNA, homozygous normal, without sickle cell mutation
Issues that could be raised:
- The fetus will be born with sickle cell anemia. Should the fetus be terminated?
- Should the parents have additional children knowing they are carriers?
Case B:
Mattie has just returned form the hospital after visiting KC, her favorite nephew. She and her family are already grieving the loss they know is coming. She has watched her only brother, Josiah, and his wife, Emma, deal with KC’s illness over the years. She feels as helpless for them as she does for KC. Josiah shook her up when he blurted out, during a period of overwhelming stress, that if they had known ahead of time, perhaps they would have chosen a different route, and that she should get tested to avoid the same suffering. Mattie knew it was the stress talking, and that Josiah would not trade any of his moments with KC, but maybe he was right about her. Maybe she should go into parenting with her eyes open. Maybe she should find out if she could bear a child with sickle cell disease.
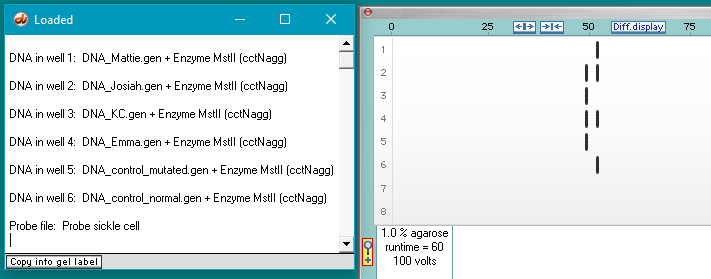
- Mattie (sister) – homozygous normal
- Josiah (brother) – heterozygous (carrier)
- KC (nephew) – homozygous for sickle cell mutation
- Emma (wife) – heterozygous (carrier)
- Control DNA, homozygous for sickle cell mutation
- Control DNA, homozygous normal, without sickle cell mutation
Issues that could be raised:
- How should Mattie react to Josiah’s situation, after she knows she has the normal genotype?
- How would Josiah react to Mattie’s situation, knowing she is normal but he is a carrier?
Case C:
Claudine and Andre Kasonga live in a small community in sub-Sahara Africa, surrounded by family and friends whose children frequently suffer from malaria or sickle cell disease. They themselves have both had siblings succumb to each of these diseases. While they both appear to be fine, they are expecting their first child and wish to know how to prepare themselves. Should they move away from the malaria-carrying mosquitoes, or wouldn’t it matter? They decide to get tested.
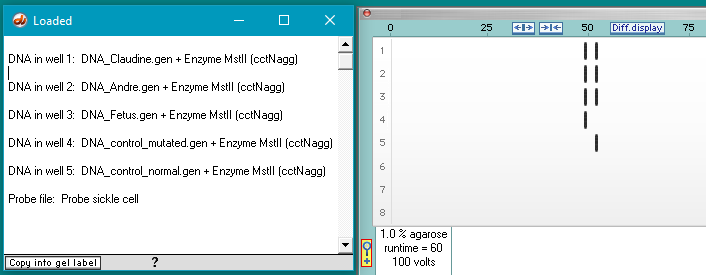
- Claudine (mother) – heterozygous (carrier)
- Andre (father) – heterozygous (carrier)
- Fetus – heterozygous (carrier)
- Control DNA, homozygous for sickle cell mutation
- Control DNA, homozygous normal, without sickle cell mutation
Issues that could be raised:
- Would the parents be justified in terminating the pregnancy because the child would be a carrier?
- Should the parents have any more children and risk passing along the sickle gene again?